We are grateful for the hardworking healthcare professionals who are working tirelessly under difficult circumstances. This page is designed to bring together resources to help our community learn, share, and connect around navigating through the COVID-19 pandemic. Catalysis will do all we can to leverage our resources and network to be part of the solution to this crisis.
Please feel free to comment on any of these posts so that we can help foster collaboration.
If you have questions or ideas on specific topics we can address, or would like to share some of your successes contact us at COVID-19ideas@createvalue.org.
It’s hard to prepare for the next pandemic when you’re in the middle of the first one. But hospitals and their PPE providers have no choice. With the uncertainties around COVID-19 and new variants emerging, healthcare providers and PPE suppliers do not have the luxury of waiting. So, what can we learn from last year that may better prepare for whatever is next? A few things stand out.
Many news headlines have been highlighting the fact that the US is not vaccinating as many people per day as they had hoped. There is a myriad of reasons, but it often comes down to lack of planning, poor processes, and flow of the vaccines into the hands of those who administer them. But there are many healthcare organizations out there who are well-versed in lean thinking and problem-solving that have created processes to achieve the necessary goals for number of people vaccinated per day. One of those organizations is Salem Health in Oregon.
Today I am joined by Team members, Pam Reznicsek and Whitney D’Aboy, from Salem Health to talk about their vaccine clinic and how they are using continuous improvement methods to meet and exceed their goals for getting their community vaccinated.
Peter Mariahazy: Thank you for tuning into the lens I’m your host Peter Mariahazy.
Peter Mariahazy: Many news headlines have been highlighting the fact that the US is not vaccinating as many people per day as they’d hoped. There are a myriad of reasons, but it is it often comes down to a lack of planning processes and the flow of the vaccines into the hands of those who administer them. But the good news is there are many healthcare organizations out there who are well versed in lean thinking and Problem Solving that have created processes to achieve the necessary goals for vaccinations administered per day. One of those organizations is sailing health or going to settle and health in Oregon today I’m joined by team members. Pam Reznicsek and Whitney D’Aboy from Salem health to talk about their vaccine clinic and how they’re using continuous improvement methods to meet and exceed their goals for getting their Community vaccinated thank you both for joining me today. Well, will each of you introduce yourselves and tell us about your role at Salem Health and your role in the development of the code vaccine clinic Pam why don’t you kick us off.
Pam: Okay um hi I’m Pam Reznicsek, I am the Kaizen Learning and Development Consultant here at Salem Health and I’ve been here at seal help about. Almost 17 years now working in primarily in the registration department and work my way into leadership and now into the kaizen promotion of this. And I assisted in the coven kind of host vaccine clinic really in the problem solving along with the revenue cycle teams, I really help develop their processes so now. How this is going, you know how do we, how do we bill and how do we actually implement streamline registration and those types of things so that’s kind of. My expertise, I also actually worked at the vaccine clinic during registration and training we brought on the National Guard, so that we have more hands-on deck to kind of help through the process and that’s where I assisted with the workflow to help.
Peter Mariahazy: Whitney, how about you?
Whitney D’Aboy: hi my name is Whitney D’Aboy I’ve been with sales health for the last 10 years and I’ve been the Manager of our Kaizen Promotion team for the last two years. I was very excited to get the opportunity to help design our clinic flow, both internally for our employees and how do we actually get our own staff vaccinated as well as how do we then replicate that out into the Community, so we can really start to vaccinate our Community Members as well.
Peter Mariahazy: Thank you Whitney you know, since you, you were really instrumental in setting it up, can you walk us through the process at a high level and then maybe you know Pam can kind of help close it out?
Whitney D’Aboy: Absolutely, and so what was really innovative and really supported the ability to get a clinic up and running, within two days I was that we, our lean office, partnered with our HIC structure, so we actually activated incident command, where we had our incident commanders we had section chiefs, including planning operations finance all of the above, right. And, and we were actually able to assign your called scribes we actually have a lean person. In our office tied to each of the different section, so that way they can really start to help each section design their piece of the COVID clinic puzzle, and so I was tagged in with planning and our goal was to design a workflow that could accommodate 2000 plus vaccines administered a day. And it was kind of funny we weren’t given a location, we didn’t know where we’re going to be doing this we didn’t know if we’d have wifi available. So epic may not have been an option, our electronic medical record, but they said high level start designing what this vaccine clinic would look like. From there, it was actually kind of fun, so we think within one day we actually found out, we had our state fairgrounds available to us. We still didn’t know if we’d had white fi so we had to think very quick and crude what is something that we could create that could move people through about 2000 plus people through in one day.
We made the process maps lots of visuals were included in this planning process and our goal is to really just keep it as simple as possible, how do we move people through. Where the process actually tells the people where to go and it as simply as possible as well, so I think there was a lot of great learnings that we had along the way again when you start out quick and crude we actually started with paper everybody was signing paper consent forms and paper co a’s and all these types of paper things, of course, that creates issues on the back end of how do we actually start to understand and When are they do for their second dose because nothing’s in the medical record of that point. What was great as we’re able to then start with something quick and crude we had paper signs up even because we weren’t sure the exact flow just yet, so when we open the clinic that day, we had everybody on paper, and then we started to just quickly check and adjust every single bit in in the beginning, so we knew we didn’t have a perfect flow because we designed it within 48 hours or less and then we were just kind of gave ourselves the grace to basically say all right we’re up and running, we had a test population of about 500 people come through and where we are trying to just understand where the hiccups along the way, and then we just quickly checked and adjusted we actually that first day identified those that had mobility challenges, how do we accommodate for them so that wasn’t something in our original design, because we were just trying to think high level 2000 people. So that’s when we started to create okay well, maybe there’s like a fast track pass where we can bring them kind of through as quickly as possible um so they wouldn’t have to stand in line we also created the
fragile population flow, where they would come in through a whole separate entrance and have their own station available to them, so that way they didn’t have to commingle with kind of more general public. And so it was really, really great to be able to have that structure in that partnership to really harness different leadership roles around the organization. To really use their expertise and how to design, something that was quick and crude and then everybody was just in that mindset of how do we just checking the just as quickly as possible so that we can just be fluid throughout the entire the entire process.
Peter Mariahazy: Thank you Whitney and I love that phrase quick and crude because then that gets handed off to Pam to get it to smooth and easy right.
Pam: Yes, so, to whitney’s point, we had the paper process right, so its first day maybe I think it was actually a little bit further than the first day. We were doing people registrations right, so there was some concerns about how do we get the records, how do we get the reporting and we need to get this into the electronic health records, so now, what do we do so that’s where I would spend a bold in with the revenue cycle team. And again just actually pulled in by the VP of finance saw me and all hey, we need to do some problem solving around road cycle, with the specs in clinic come with me and so kind of off we went and through that day we kind of did a lot of Problem Solving the team was working very hard to get those registrations in there and the team on site like scanning in the documentation, so we can have those records to be able to send out for reporting and make sure that we got all of those things going and then really just thinking about Okay, now that we know a few days in about how many people are coming through now how do we start planning and streamlining the process so I actually helped probably within the first week of vaccinations, we were we were steep we were full steam ahead right, we were seeing you know over 2000 people a day the governor’s like we need to keep moving Oregon at that point. When we started our clinic was about 25% of the vaccines that we had received as a state were actually given in the states, and so there was a concern that we may actually lose those because you know they do have a time limit and for storage and things like that so she partnered with us, as well as Marion Marion county has been kind of our partner from the launch. And we got resources from the National Guard to actually help even continue growing and so that’s where I came in was helping with now that we have National Guard, how many people do we really need to have for this flow. So doing some timing, we have kind of two registration flows right so we’ve got one that we’re really encouraging the Community to do where you can sign up for my chart schedule ahead of time get all your documentation comes in your about three and a half minutes and away you go your vaccine first is our other workflow where people don’t want to start the my chart they’re doing paper basically handwritten paper that we enter a full registration into our system takes about anywhere from 10 to 15 minutes for those full registration. So how do we manage the flow between those two? Registration close rate so, on average, you know how many people are coming in, so we could actually take the numbers and kind of plan out the staffing for the registration team. Based off of the cadence of check ins and things like that, so that. we knew how many from a scalable perspective if we were to say now do 3000 people how many people would be needed. When he was doing similar work at the same time around, how many people we needed a vaccine versus watching and we had multiple different roles that we have within the clinic so that’s kind of how we help support it and I would say that one of the key things was replicating the clinic kind of workflow like we had started our own internal vaccination clinic and we vaccine we’ve actually added our organization very quickly. So I would say, for others, thinking about that you have a flow, that is in existence if you’re vaccinating your people, so there is something there that can actually be used as a model. Even though we stood up the thing in two days we kind of had a structure that we can build, I would say, maybe three or four days just for our own team that we had been using for two weeks, and also revising so again it’s really starting something. To Whitney’s point directionally where it needs to go and then, as you build the structure, you can kind of check and adjust I would say it’s continuing to check in and just you know go.
Peter Mariahazy: Thank you Pam. So you kind of teed up the next thing so I’m going to ask each of you to kind of give us give us. If you if you’re starting this process now or you’re working with a whole new organization that hasn’t done this yet give me the top two or three, obviously people can only absorb so much at a time, two or three considerations that they need to consider in developing the process. Whitney, what do you think what’s the top two or three things they really need to think about?
Whitney D’Aboy:I think what really made our successful with that partnership with the HIC structure and so having those different leaders throughout the organization with their different expertise at the table, helping with their lens to help design what this could look like, I would also say we need to vaccinate, we need to vaccinate quickly so how do you remain as quick and crude as possible until you get kind of an understanding of what the flow could be like but as you’re checking and adjusting and then you can really start to move into what does so know of this process, look like.
Peter Mariahazy: Great and Pam, what are the top two or three things you tell somebody who’s just about to set it up?
Pam: I would echo the quick and crude. I was thinking keep it simple, so you know, for registration, I would say the for registration here at Salem Health we get a lot more information so what are the minimal things that we actually need? So, really thinking about what you need in the workflow and just look at the bare minimums and start there because when you start with the bare minimums of like what do you need to actually deliver the vaccine. And me all the things that are needed for the vaccine and then build upon it, because once you’re using the process you’re going to learn and evolve I would say. It really speaks to our lean journey in Salem health that we like frontline staff and leaders it’s not just a few people doing this planning it’s literally everyone who’s working in the workflow is checking and adjusting and Problem Solving as they work so.
Peter Mariahazy: I was just gonna say Whitney you kind of talked a little bit about starting the process and doing you know process mapping and bringing the various people together that are experts. So anything else you can think of that just got you started and getting the thinking going quickly?
Whitney D’Aboy: What was really great was we actually had a very, very high level process map right, so we need them to somehow get their paperwork and then somehow, you know. There was conversation of okay well where do they fill out the paperwork? And then we’re like well let’s give them a pen and they can do it in the car right, so we just had a very, very high level, and then, once we identified our space we had a printout of our process map and we actually took it there with us to walk it, how would this actually physically look in this space? And so that was really instrumental we did that on like day one design day to walk it and day three is the day we launched. So that’s where it was just a matter of we didn’t overthink it like I said we didn’t even think of like oh gosh people with mobility challenges, how do we accommodate. If we had spent all the time on Monday baking and all the What if scenarios, we would have never been able to launch and so that’s where I would say that walking the space and then that afternoon, so it was a Tuesday afternoon we actually started being like okay well if this is going to be here let’s start you know, putting tables out, so we can really start to visualize it. And then, again we had every single section chief from our HIC structure, whoever was on that week President, so they can like our safety officer was thinking like okay well if this is where the tables are going to be and we’re going to have people walking this distance, how do we make sure that they don’t trip over something right so she kind of had her lens going of what would make sense as we’re designing So while we had a high level visual what really made it important, and I really think this enforces the concept of go and see is we were designing it while we were seeing it so since we didn’t have the people on site, yet we were able to kind of all let’s move this table back here, and what we had come to the line move this way and we can move this over here, and so we truly were just did we had a again that high level thought in our minds, but we were able to just design, all together, as a group, on the site, which is very, very valuable.
Peter Mariahazy: I think it’s great that is that you started the process before you even knew which space you’re going to end up with, I mean that’s what’s to me very intriguing is to say that, and so anything Pam to add regarding starting the process, I know you can have came in a little bit downstream but.
Pam: No, I think we covered most of them, I would say that you know once things have got their flow we’ve created standard work on things right, so their standard work for people doing vaccines standard work for people who are drawing vaccines ahead of time, so we have people who are preparing the vaccines and kind of distributing them out, and so, and then visual management. And I would say again in the background, the incident command structure is really keeping track of data right so. How many people are flowing through what’s our supply look like, how do we need to check and adjust so it’s a system in the background that’s informing the flow in the actual operations so.
Peter Mariahazy: So give us give us a couple of the challenges you faced along the way, what are some of the things that you went oh geez and a really kind of caused you to you know sit down and need a cup of coffee?
Whitney D’Aboy: At the beginning, and when we were doing so many quick and crew changes right so we’re like oh gosh, we need to set up this, we need to do that and it was hard to keep everybody informed of all the changes so it really reinforced the concept of like a visual quick and easy board of some kind. Or even huddles right So how do we take the day off like okay guys, these are the changes we made yesterday, this is why were they were changed and keep in mind, you know if you if you think of more great ideas put them over here, right? Those are some of the things I wish we thought of it at the moment, some of our basics and principles right and so that communication breakdown was visible every single day as we’re like oh crumbs yep that didn’t get communicated to you let’s let me keep get you up to speed, so that way we don’t stumble over the same stumbling blocks, we did yesterday kind of a thing, so I would say to help prevent some of those communication barriers absolutely making any of those kind of quick and easy ideas visible and then, how do we include it in a huddle we eventually did institute something to this degree, it just took us a good five days before of stumbling every single morning. And before we finally got something in place to actually but to have that in the beginning, would have been would have been much better, much smoother.
Peter Mariahazy: So Pam other than them having to use paper forms what were some challenges you experienced?
Pam: I would say that was kind of the big thing is oftentimes revenue side, like everything happens, you know for the patient, while they’re in house and then the revenue cycles obvious an afterthought. And being someone who has come from the revenue cycle I get that so but I think the benefit, we have an even though, like to Whitney’s point, though there were things that were missed and things that may have been changed, I think our team has a lot of grace with one another to know that we’re doing this for our patients and it’s really about getting them vaccinated like we care about our Community. And so we’re going to do what we need to do in order to care for them, and then we will do our best to figure out how to make it because we know that it’s not going to be perfect straight up. Again, I think that through all of the incident that commands that we’ve had from David, we have learned that it is not going to be perfect right away but that we will come together and we will problem solve and use our tools to actually make it better, and so, in the end, hopefully to produce something that others can then replicate and not have to stumble nearly as much.
Peter Mariahazy: Excellent. So in retrospect, you kind of look back on you know the quick and crude right. Whitney what was the one single biggest learning that you got as this process rolled out what’s The one thing that jumps out to you?
Whitney D’Aboy:I think it’s really impressive how much our organization can do on a short timeline if we’re given the goals and it it’s amazing how people can come together and design quickly and deliver something I don’t think we ever thought, like you know, five years ago that this would ever be a reality. Where our organization is used to lean, to the point where like hey let’s just quick create other process map this let’s make a visual right, so I think it’s just it’s my biggest learning is just how great it is that we can, if we challenge ourselves if we push ourselves, we can actually do so much in such a short amount of time and it’s such a great outcome for the Community.
Peter Mariahazy: You know that sounds like it’s a real testament to culture right the culture, the organization lays the foundation, and then, whatever the world throws at you, you guys are together to handle it so Pam what’s the single biggest learning for you?
Pam: We talked a lot about the HIC structure, I would say the way we do our hospital and saying command structure may look a little bit different because it is kind of a standardized thing, but our lean principles have allowed leaders to kind of make things their own so like the planning lead planning section team can those teams can actually develop and build things that are important for that team what is that visibility and so, though, though we give structure oftentimes we use our lean thinking to make it work with and I think that’s one of the things that was an Aha moment for me, in in this last year. and just working a lot more with incident command is how much we to your to Whitney’s point how much we can do when we actually come together and use our thinking and that kind of structure of like you know, making things visible walking the processes going and seeing you know, creating visual management and standard work around things like we do it very quickly. And so, how do we now, though, we can do something as big as this, how do we know why this organization and I think that there’s some great learnings that we can do from this, as we continue to grow our own culture and I know for sure.
Peter Mariahazy: That’s a that’s a wonderful observation, so you know Whitney you get a phone call from somebody across the country what advice, do you give them who’s still developing their vaccine process.
Whitney D’Aboy: I would say don’t overthink it. Just try something start with something and start running and seeing where it goes, if you start overthinking it you think of again all those What if scenarios, and you’re spending too much time designing and you’re not getting vaccines and arms right that’s the ultimate goal So how do you do that as quickly as possible, so if you if you’re overthinking it and you’re slowing yourself down and just you need to start with something and just start running.
Peter Mariahazy: Ties to Pam’s keep it simple right just you know progress over you know paralysis so Pam whitney’s just finished giving that advice transfers the person to you, what do you say to them to give them advice?
Pam: A first Whitney’s advice is great so definitely take that into consideration. It’s about continuous improvement, right? And I think at this point, a lot of healthcare organizations, you are doing, vaccines within your own walls so how do you now take it a little bit further and challenge yourself, again we took a big challenge we were like 2000 a day. It doesn’t have to be that big I think we can probably move this needle quite a bit, even if we’re doing smaller challenges. But if most healthcare organizations are just kind of taking that leap to say how can they, how can they now support their community and the people out there that they’re caring for. Just a little bit take what you’ve learned and improve on it a little bit and, over time, we will have everyone vaccinated you know, in a short order so great.
Peter Mariahazy: So, as we kind of start winding down Whitney any final thoughts, you want to share with our listeners?
Whitney D’Aboy: Um I would say, this is a great opportunity to start thinking about so we’ve been open and operational for about three weeks now, a little over three weeks and so now we’re in the head we start handling second doses and more people right, so we are accepting 2000 plus up to 3001 day people. So now we’re still anticipating 2000 people coming through last the 3,000second doses So how do we now have a scalable model that can get up to five 6000 doses a day. And so really thinking through what’s that scalability I know Pam has been talking a lot about ratios right how many registrar’s to how many vaccinators. So really kind of stretching our thinking in that way, as well as. What does snl of this look like right we can’t have our HIC structure and every single lean team Member out there every day for the next nine months or however long it might take until everybody in our state is vaccinated. So that’s where we really had to start thinking of the permanence who is truly going to be that operational director over some of this work, and you now have kind of spiders out to different clinics and things like that So who is the ultimate kind of person over this now that we’re sending data structure. And in our incident command and then who are those kind of interim and all of this has to be interim because we’re not gonna have a vaccine clinic up five years from now, I hope, and so, who can we kind of start putting in place and really start to create that structure where there is a hierarchy where decisions and they can get more of the sustain and operate, huddles going more efficiently, quick and easy words, how do we create more? Strategically that visual management board right we’re using our key metrics and how we’re doing each day. And so that’s where our next kind of focus is going, is how do we handle first and second dose is flowing through our clinics and as well as how do we start getting more of that snl structure so that way, the rest of us can try and start getting back to some of our other responsibilities.
Peter Mariahazy: Thank you Pam any final thoughts, you want to share with the audience?
Pam: Um I would say, you know for us we’ve had some barriers with you know, lack of vaccines so I see that that’s probably going to be something you know with bigger structures, like that so don’t be surprised if some of those things happen so you know we have we were flexing our model. As we go and so keeping those things in mind and then again for us, yes, like the incident command structure pulls a lot of our leaders so most of our executive team is involved in a rotation actually all the executive teams involved in a rotation, as well as our all of our directors. And so, you know that is pulling from operations so it’s very important for us to now that we’ve got this running and know that we’ve got a process, how does this become its own operations, and then we can now focus back on regular operations and the clinic has its own leadership and sustainment moving forward.
Peter Mariahazy: That’s excellent. That’s a great way to kind of close it out, so thank you both for joining us today. And really appreciate you sharing the work on the COVID-19 vaccine clinic at Salem health.
For our listeners, please visit our code 19 resource page at create value.org to find more information and learning about navigating around the code 19 pandemic.
There is also information on YouTube specific to the Salem clinic stay tuned for more episodes designed to help healthcare leaders support their organization on a journey to operational excellence.
New York City-based Mount Sinai Health System researchers used federated learning, an artificial intelligence technique that protects patients’ privacy, to analyze EHRs and better predict how COVID-19 patients will progress, according to a Jan. 27 news release.
The federated learning technique has the potential to create machine learning models that go beyond a single health system’s information without compromising patient privacy. Using the model and data from EHRs at five separate Mount Sinai hospitals, the researchers were able to predict mortality in COVID-19 patients.
Testing remains uneven across states and communities, and case counts and death tallies are considered to be too low and incomplete, according to the Jan. 22 report.
“A lot of the reason we have struggled in the U.S. is because we have such a diffuse approach to healthcare,” said Beth Blauer, executive director of the Johns Hopkins University Centers for Civic Impact. “It has led to states implementing things pretty differently, and it has made it very difficult to create an apples-to-apples comparison.”
The safe and prompt administration of the COVID vaccines is one of the most critical issues today in global public health. In this 90-minute panel discussion moderated by Mark Graban and hosted by Value Capture and KaiNexus (in partnership with Catalysis), healthcare leaders from the private and public sectors will share their experiences with the COVID vaccine administration processes — what is working, what is not, and how Lean is helping make these processes better. The objective of this webinar is to share the lessons these leaders have learned and continue to learn, in near real time, so that others dealing with their own vaccine administration challenges can benefit from and contribute to this discussion. We anticipate informative and lively discussions, with ample opportunity for Q&A.
Panelists:
Secretary Daniel Carey, MD
Secretary of Health and Human Resources
Commonwealth of Virginia
Penny Iannelli
Chief Transformation Officer
UMass Memorial Health Care
Lisa Malosh
Senior Director, Organizational Improvement
Presbyterian SeniorCare Network
Shlomit Schaal, MD, PhD, MHCM
Professor and Chair of the Department of Ophthalmology & Visual Sciences
UMass Medical School
President
UMass Memorial Medical Group
Senior Associate Dean for Health Strategies UMass Medical School
Or find The Lens, by Catalysis wherever you get your podcasts
The COVID-19 vaccine is on the minds of everyone around the world. Here in the US the vaccine roll out can be very different depending on state, county, or event city. We hope that by sharing work that is going on in healthcare organizations we can help others that may not be as far along in the roll out, or help others improve their processes.
Today I am joined by team members from Torrance Memorial Hospital, a member organization of the Catalysis Healthcare Value Network. We have Jeremiah Hargrave, Leah Romine, and Christopher Bacon who will share about the COVID-19 vaccination process and how it was developed.
In this article many frustrated Florida residents, including John Toussaint, share their frustrations about the process for signing up to get a COVID-19 vaccination in their area in letter to the editor of the Naples Daily News
We have seen proof that there is a better way. Catalysis Healthcare Value Network member organization, Salem Health in Oregon, shared how they have been able to work with local and state agencies and stand up a COVID-19 vaccine clinic open to the public that has been vaccinating thousands of people per day. Learn more about the vaccine clinic.
Salem Health shares its initiative to provide COVID vaccines publicly. They share their Lean thinking, PDSA problem-solving methods, and visual management systems.
Houston Methodist is offering its employees a $500 “hope bonus” if they meet several eligibility criteria, including getting a COVID-19 vaccination, President and CEO Marc Boom, MD, said in an email to employees, which was shared with Becker’s Hospital Review.
Workers can look forward to the bonus in early March, according to the email.
“This bonus is a thank you for your perseverance throughout a difficult 2020 as well as something to look forward to, to provide hope, during the next couple of challenging months,” wrote Dr. Boom.
Houston Methodist said eligibility criteria for the bonus will include getting the vaccine, and the human resources division will notify employees of the additional criteria soon.
Seattle Cancer Care Alliance, a Catalysis Healthcare Value Network member, put together an expensive FAQ to share with their staff about the COVID-19 vaccine.
Our latest U.S. tally includes 556,208 shots, with details from 40 states and territories
The first Covid-19 shots have been given to more than 1.8 million people in five countries, according to data collected by Bloomberg. It’s the start of the biggest vaccination campaign in history and one of the largest logistical challenges ever undertaken.
Vaccinations in the U.S. began Dec. 14 with health-care workers, and so far 556,208 doses have been administered, according to a nationwide tally from the Centers for Disease Control and Prevention. Those numbers are expected to surge in coming days with the distribution of a second vaccine by Moderna Inc. Bloomberg is also tracking doses at the state and territory level to give a picture of how the rollout is going nationwide.
Most scheduling through employee/occupational health
ACTION: Need a “call list” to fill in for no-shows
People were showing up at a time different from their scheduled time. ACTION: Create a plan to deal with this situation
ACTION: Need a list that prioritizes who “should” get a shot first
ACTION: Recommend polling for the list of volunteers to get the vaccine
Issues encountered:
Needles were getting bent and/or dull when inserted into the vials for a draw.
ACTION: Have spare needles on hand
There have been some reported reactions by those on our call today (severity unknown)
ACTION: Have Code Team ready
Delivery of vaccine to the nurses
ACTION: Create tight communications with the area (pharmacy) preparing vials and the nurses administering doses to keep product flowing and a pace of administration.
Some vials had more than 5 doses. OK to use up all product in vial message came out today from Pfizer
NOTES:
Need new workflows for when Moderna vaccine arrives. ACTION: Begin designing new workflows now
Patients are receiving a piece of paper as an official document of vaccine
Patients are being required to sign a consent form like the flu vaccine
70% of people on the sharing call stated they have begun administering the vaccine to staff
80% of people on the sharing call stated the organization had a formal communications process on the vaccine
Over 80% stated that the perceived willingness from front-line stall about getting the vaccine rated it 4 or 5 (0-5 scale. 5=Very Willing). Improved opinion from the last session. Not a scientific study.
Anyone willing to share other notes or action items, please share with us.
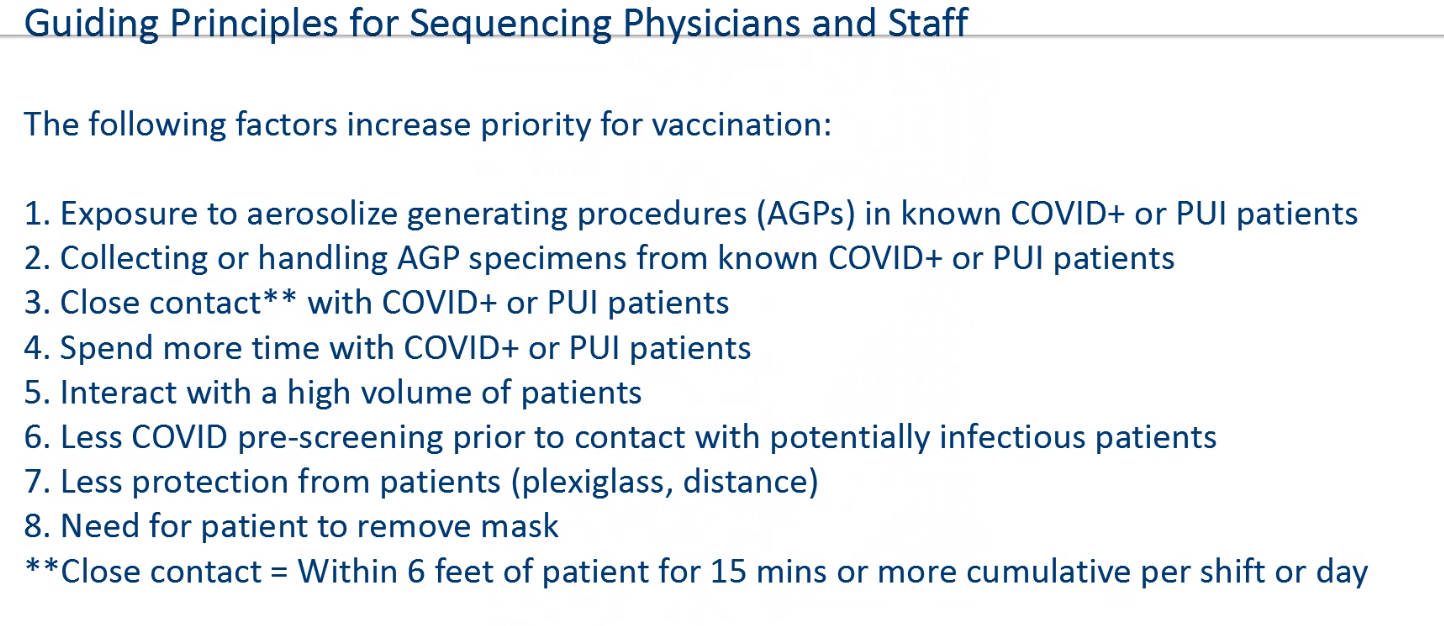
Shipments of the COVID-19 vaccine have arrived at many healthcare organizations and are anticipated to arrive in many more within the coming days. Now comes the question: which healthcare staff members should have priority? There are very few guidelines out there, which means healthcare organizations have to determine this on their own.
Some of our Catalysis Healthcare Value Network members have shared their work.
This is a framework from a physician group:
Here is a link to a prioritization plan from a health system:
Facing challenges ranging from misinformation campaigns to public hesitancy, healthcare leaders are sharing the messages they want to spread to encourage COVID-19 vaccination and some of the strategies their organizations are taking for marketing campaigns.
Here are seven messages and marketing campaign strategies that physicians and healthcare organizations want to push for vaccine education:
Trucks filled with Covid-19 vaccine vials pulled out of Pfizer Inc.’s Kalamazoo, Mich., production plant on Sunday morning, part of one of the largest mass mobilizations since the country’s factories were repurposed to help fight World War II.
The effort to vaccinate the nation relies on chemists, factory workers, truck drivers, pilots, data scientists, bureaucrats, pharmacists and health-care workers. It requires ultracold freezers, dry ice, needles, masks and swabs converging simultaneously at thousands of locations across the country.
To work, every one of the many and complicated links of the chain has to hold.
I was scrolling through Instagram in early August 2020 when I saw an advertisement that caught my attention. Usually, I swipe past these without a second glance, but this was for the Pfizer-BioNTech coronavirus disease 2019 (COVID-19) vaccine trial. It was recruiting participants for the highly publicized phase 3 trial of a new vaccine, BNT162b2, that had shown promising results earlier in the year. As a nurse and researcher who has encountered social media recruitment in my own work—and has closely followed the COVID-19 vaccine trials—I was curious to see how Pfizer planned to convince 30 000 people in the US to volunteer. I clicked on the advertisement.
The recruitment website (https://www.covidvaccinestudy.com/) was nicely designed with bright photos and thoughtful messaging about the trial. I intended to look at the recruitment approach, but found myself instead thinking about how important it is for people to participate. In the US, as of September 2020 COVID-19 had been diagnosed in nearly 7 million people and had killed more than 200 000.1 A vaccine could save lives and stop the spread of the virus. Volunteering for the trial felt like an honorable thing to do—and the 50% chance to be randomized to the vaccine early seemed equally compelling to me as a practicing nurse. Before I left the website, I entered my contact information to be considered for participation.
The cost of getting a standard COVID-19 test at hospitals varies drastically by state, according to a nationwide study conducted by Hospital Pricing Specialists.
For the analysis, Hospital Pricing Specialists reviewed billing data from 2,862 hospitals across the U.S. to determine the average price of a nasal swab COVID-19 test. The claims reviewed had the Current Procedural Terminology code 87635.
The state with the highest average cost is New Jersey at a price of $302, whereas the lowest cost is in Maryland at $62.
Below is Information from our latest COVID vaccine sharing session by network members:
• The use of the Project Management Office and the Process Improvement teams to design and adjust new workflows are going great
• Will need to stagger inoculating staff in case of adverse reaction
• Inoculate staff at the end of their shift instead of the beginning due to some adverse reactions
• Security of the vaccine is a significant concern. The vaccine will be a high theft item. Secure the vaccine where the Class 1 or Class 2 are stored.
• Some are tracking the COVID-19 vaccine using the same method as the flu shot. Some are using Employee Health and their system.
• Essential worker populations like police and firefighters will need to be staggered for inoculation too
• Need better communication internally and to the public. Get messages out early and via multiple channels to avoid inundating the call centers.
• Involve your Compliance people early in the new workflows and processes
• Need an “inoculation delivery” plan. Example: Are you going to “preload” the needles or draw at the time of delivery?
• Plan on a daily or more frequent inventory status reporting process for leadership
• Most are planning on using all their vaccine on the first dose and then using later shipments for the second dose
• Some were planning on handing the patient a document as evidence of the inoculation versus just recording in the EMR. This is in case the patient goes somewhere else for the second dose and to minimize the calls coming in to assist help people access their medical records.
• Your EMR vendors are creating workflows and reports to make this easier.
If you are diagnosed at Lee Health in Fort Meyers, Florida, with COVID-19 symptoms, you’ll be given a blood thinner as part of the standard treatment protocol. That’s because Lee’s physicians used the data in their Epic healthcare software to verify early reports linking COVID-19 to blood clots.
Their analysis showed that otherwise healthy patients with the virus are three times more likely to develop fatal clots.
Lee Health’s experience shows how observational data help scientists discover new connections that can prove critical to advancing patient care.
Observational data allow you to look at a specific variable, such as “COVID-19 positive,” and determine quickly whether there is a link to a specific clinical condition, such as developing a blood clot. It also helps get lifesaving guidance into the hands of doctors and nurses quickly.
The gold standard for clinical evidence is the peer-reviewed, randomized controlled trial, but that process can often take years. While this approach is necessary for novel treatments and vaccines, we can’t wait years to learn more about COVID-19.
To better treat people in this pandemic, we need to learn everything we can about the virus as quickly as possible. Observational data provide clues that can save lives today and help researchers understand where to focus for tomorrow’s peer-reviewed studies.
In May, the Epic Health Research Network, or EHRN, was launched in an effort to make observational data available to all physicians and researchers. EHRN is a collaborative journal for the 21st century using observational data from participating healthcare organizations. It’s a platform to share novel discoveries from a large patient population, and it is open to any healthcare organization or researcher to submit their observations or collaborate on future possible studies or treatments.
EHRN also offers insights and ideas Epic researchers have observed based on de-identified patient data that Epic customers have collected over decades.
Today, data from more than 50 million people are helping drive insights shared through EHRN, and we expect that number to grow to 200 million.
With Epic customers’ permission, EHRN is investigating how patients have been affected by the COVID-19 pandemic.
In response, Epic has plans in place to work with healthcare organizations to better understand how these decreased screenings might affect future cancer rates in our country.
EHRN is not alone. Preprint platforms such as Dr. John Inglis’ bioRxiv and medRxiv do something similar. They are designed to promote the rapid sharing of knowledge to respond quickly to emerging health crises, like COVID-19.
As noted in a recent study posted to medRxiv, “There is a paucity of data that can be used to guide the management of critically ill patients with coronavirus disease 2019 (COVID-19). Global collaboration offers the best chance of obtaining these data, at scale and in time. In the absence of effective therapies, insights derived from real-time observational data will be a crucial means of improving outcomes.”
We know there are many questions that health experts, policy makers, and individuals need answers to as we all battle COVID-19.
As one of the nation’s largest healthcare records companies, Epic takes its responsibility to help discover and share new information seriously. We encourage you to visit EHRN and send our observational data team your questions.
Together, we can uncover new insights about the virus and ultimately save lives.
Judith R. Faulkner is founder and CEO of Epic.
John Toussaint, M.D., is executive chairman of Catalysis, a nonprofit education institute, CEO emeritus of ThedaCare and a member of Epic’s board of directors.
Safety is an essential focus of healthcare organizations on the journey to organizational excellence. For Hennepin Health in Minnesota, patient and staff safety is a top priority. Consequently, it comes as no surprise that when the COVID-19 pandemic hit they chose to use their problem-solving skills to come up with a creative way to approach PPE use and safety.
At the start of the pandemic, concerns about PPE and risk of exposure was at an unprecedented level. In response to this, Hennepin Health created the PPE Buddy program – to protect their patients by protecting their staff. These buddies, who were staff from areas that were required to shut down (physical therapy, diagnostic imaging, etc.), helped provide extra support for all staff in donning and doffing PPE with COVID-19 positive or rule out patients. So how did they set up this program and make it successful?
Frontline health care workers are at high risk of contracting severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19).1 Personal protective equipment (PPE), including N95 respirators (N95s), is essential for prevention of COVID-19. The Centers for Disease Control and Prevention recommends that health care workers dispose of N95s after a single patient encounter. However, it recommends N95 extended use (wearing the same N95 for multiple patient encounters) and limited reuse (storing an N95 between encounters for use over multiple encounters) during critical PPE shortages.2,3 There are limited data regarding N95 reuse and extended use. Existing studies were conducted in laboratories, not clinical environments.4,5 Inadequate supplies of N95s have forced many emergency departments to implement various N95 reuse and extended use policies but without empirical evidence of their effectiveness. We examined the prevalence of N95 fit test failure while reusing 2 common types of N95 masks.
The COVID-19 pandemic turned many of our lives upside down and inside out, which highlighted the need for leaders to be able to help their staff by translating behavior and shifting thinking to help keep work environments positive for everyone. Today Kerri Burchill, Organizational Development Leader at Southern Illinois Health, will share a methodology that leaders can use to help staff who are struggling in the rapidly changing environment that COVID-19 has presented.
In this episode you will hear examples of conversations around tough topics facing healthcare workers across the country. These scenarios demonstrate the 4 step process that Kerri Burchill teaches.
Patient Volumes have not returned to normal in most health care organizations in the U.S. One of the main reasons is people are scared to go to the doctor’s office. We might get infected from workers, other patients, even doctors. To assure it’s safe look for the following four things.
Is a drive through visit available? Everyone has heard about drive through testing; what about a drive through doctor’s visit? At the Christie clinic, a multispecialty physician clinic in Champaign Illinois, urgent care visits have been completely redesigned. As the number of COVID cases diminished at the beginning of May, non-COVID patients weren’t coming in for urgent care visits. Patients thought COVID patients might be seen in the clinic increasing their risk of contagion. Christie clinic created a process based on a “care at the curbside” idea from staff. They dedicated an urgent care clinic to COVID curbside care and started seeing patients in their cars. When symptomatic patients called their primary provider at other sites, they were directed to the COVID designated urgent care center. Providers, mostly advanced practitioners, in protective gear stood in a makeshift car port on the side of the building and not only tested suspected COVID patients but also examined them. If lab or x-rays were ordered, patients entered the clinic through a side door and donned PPE given to them by staff. No other patients were exposed because they didn’t check in at the desk and they didn’t sit in the waiting room. Patients went directly back to their car after testing to wait for results and prescriptions. By mid-May the waiting room at the urgent care clinic was empty most days despite seeing close to the same number of patients each day.
Do you have to wait more than 5 minutes for anything? If the waiting room is even half full there is a problem. In addition to urgent care, Christie runs many outpatient clinics. What they learned from the urgent care center were applied to the clinics. Doctors realized that the traditional way of checking in patients was an infection waiting to happen. At peak hours, as many as 10 people were standing in line. A team of medical assistants (MAs) and nurses had the idea to prescreen patients on the phone thereby reducing the face time in the clinic. They could easily gather information before the patient arrived at the clinic and speed the visit process. The goal was to have no one waiting anywhere. Pre-COVID, the MAs would room the patients. It took 11 minutes. With virtual rooming the day before, they reduced that time to 3 minutes. They gathered the usual information including medication reconciliation, allergies, med/surg history and chief complaint without seeing the patient. The result: 70% of the patients were prescreened. As of June 15th, prescreening has been more difficult due to people returning to work and not being available, but still the rate has been maintained at 60%.
How many times do you have to register? Utilizing the principle of one-piece flow, patients were instructed to come only 5 minutes before their scheduled appointment unless they had ambulation issues. Pre-COVID all patients had to register first at central scheduling at Christie’s large multispecialty clinic. There are 115 physicians and 85 advanced practitioners covering 40 departments at all of the campuses. That could take several minutes waiting in line. Then they had to register again at the specific specialty office. Then they sat in the waiting room. But the Christie team that included staff from clinical serves, facilities, and business services created a new process in which there was fast check-in at the clinic, meaning no stop at central scheduling. For return patients this takes 3 minutes, for new patients about 5 minutes. The patient goes directly from registration to the exam room therefore no public waiting.
Is a video visit available? Outpatient visits moved to phone visits at Christie Clinic early in the pandemic but have now transitioned to video visits. About 20% of all visits are virtual. Video visits have had unintended positive consequences. Providers who were chronically behind in their daily schedule began to intersperse video visits with face-to-face visits. This allowed them to catch-up as the video visits were usually check-ins for follow-up, which were less intensive and could be accomplished faster than face-to-face visits. With patients arriving only 5 minutes before their appointment and doctors generally on time, patients didn’t see each other in the waiting room or anywhere else along the way. Some patients did not want to be seen in the clinic despite the above processes designed to protect them. Physicians have realized how effective video visits can be. A physician recently commented, “I can see where the patient lives, meet their cat, and have a more personal connection, I could never do that at the clinic”. Pre-COVD Christie clinic saw 2200 patients a day as of the week of June 15th they were at 2000 +per day and increasing.
There are some important lessons from the Christie experience that are applicable to all providers anywhere. Flow management is one. Flow was at the center of the work in curbside care, registration, virtual pre-visit, and even video visits. Whether patients were driving up in cars or arriving immediately before their scheduled appointment, flow was the key to not being exposed to patients who might be sick. Improved flow required doctors to change. Standing in car ports waiting for patients and in car examinations is not usual physician practice and seeing patients on a video screen isn’t either.
They kept constant focus on reducing wait times. Every improvement reduced or eliminated waiting and therefore, reduced contagion opportunities. At the same time overproduction was reduced. Single registration is a great example of eliminating nonvalue added steps in a process.
Leaders and clinicians applied the fundamental principle of customer value and embraced radical redesign ideas over incremental change. The change in thinking led to the remarkable work at Christie Clinic. The work is fluid, however. Changes in the financing of care allowed Christie to innovate. Medicare early in the pandemic began reimbursing video outpatient clinic visits at the same rate as face to face. Most commercial insurers followed suit. This has allowed for the continuation and potential growth of video visits. Some clinics in Northern California are reporting as many as 40% of visits are now virtual. But will this financing be continued?
The innovations at Christie are facing other barriers. As the temperatures have risen this summer, providers are complaining about standing outside in the overheated car port. Winter will be a different challenge. But front-line design teams are well versed in applying PDSA cycles to improve the standard while capturing new staff ideas. In this time of crisis every new idea may have a chance to be tested and our old thinking about care delivery forgotten so we can create better and safer ways and follow the lead of Christie clinic.
Before Covid-19 pandemic struck, the U.S. health care industry suffered more than 550,000 work-related injuries and illnesses per year, or 150,000 more than any other industry in the country. Therefore, it is no surprise that health care workers have been harmed at tragic rates during the Covid-19 pandemic. According to the U.S. Centers for Disease Control and Prevention (CDC), as of June 4, 72,346 U.S. health care workers had been infected, a figure it acknowledges is an undercount. A comprehensive national analysis indicates that almost 600 health care workers have died.
Every instance of a health care worker being harmed on the job is preventable. Every single one. So it is time to finally take the safety of health care staff seriously. It is time for the industry to go from the worst to the first in safety. A few visionary leaders and organizations have set out on that course and proven that it is possible. Drawing from their practices before and during the pandemic, we offer five leadership imperatives.
Catalysis Healthcare Value Network member, Cleveland Clinic, has compiled information about creating a safe workplace for healthcare and other industries.
The COVID-19 pandemic has created a number of new challenges, especially for businesses looking to reopen. While managers and employees may feel a sense of urgency to get their business back to normal as soon as possible, there are new guidelines and revised practices that should be followed to allow for a safe, stable return.
These resources will help you through the key steps of reopening your business in the wake of the COVID-19 pandemic, including:
Making sure your facility is fully clean, disinfected and equipped with a blueprint for maintaining safe conditions.
Setting up a support system in place for employees as they return to work and adjust to new realities and emotional challenges presented by the COVID-19 pandemic.
Creating a plan for a safe work environment that protects employees and customers alike from risks connected to COVID-19, including exposure and transmission.
March 1, 2020, marked the first confirmed case of COVID-19 in New York City. It was not long before the disease had reached epidemic proportions. As cases surged, NYC Health + Hospitals (NYC H+H)—the United States’ oldest and largest municipal health care delivery system—began providing care to many, many patients fighting for their lives. Soon, it became clear that our community represented, essentially, the very epicenter of the epicenter of this terrible outbreak. NYC H+H has a rich history of responding to a wide range of infectious disease outbreaks, but the impacts of COVID-19 have exceeded all modern-day epidemics, emerging as the worst public health crisis in a century.
At its most fundamental, our challenge has been a race against time to open more hospital beds, onboard more staff, procure more equipment and supplies, develop new systems, and above all, save lives. Just as fast as these resources were brought online, the ongoing surge in demand consumed them, effectively testing every facet of our health care system, from postacute care to ambulatory care to (most intensely) our 11 acute care hospitals. COVID-19 created patient loads well beyond the system’s baseline capacities, especially in intensive care units (ICUs). From March through May of 2020, NYC H+H admitted 10,437 patients with confirmed or suspected COVID-19, including more than 2,000 patients to the ICU.
This post serves as the introduction to a series of articles describing how our system grappled with this unprecedented crisis. Our hope is that our early experiences may offer useful lessons for those facing the pandemic’s ongoing and future threats—health system leaders, policy makers, elected officials, researchers, patients, caregivers, and clinicians, among many others.
The worldwide spread of COVID-19 has caused a great deal of uncertainty in many areas of our lives. The change has impacted our work lives, our home lives, and everything in between. Frontline healthcare workers have been working tirelessly to save patients and adjust processes to ensure safety, administrative staff are working from home or furloughed, and businesses everywhere are working to find new ways to meet customer needs so they can stay afloat. No matter what your specific situation is, we all have one thing in common; we are trying to find ways to persevere through the uncertainty and move forward.
Below are strategies from our team that they have found helpful in the midst of challenging ambiguity.
Many of our work habits and processes have been disrupted due to COVID-19. Some important questions come to mind as our organizations think about the future: How will we do our work? What should we return to, what should change, and how will we determine a new norm?
Kaiser Permanente shares their playbook for resuming operations. As COVID-19 restrictions begin to lift, this playbook is meant to offer useful tools for you and your leadership teams to make your workplace as safe as possible and support your employees in the best way possible.
Jeremiah Hargrave, Process Improvement leader at Torrance Memorial in California, will talk with us about how they were able to help meet two core strategies; no layoffs and meet PPE needs by practicing their core values and continuous improvement practices.
The May 8 IFC policy changes are intended to provide some financial protections to ACOs while limiting the potential for windfall gains. The IFC removes COVID-related costs from MSSP performance year expenditures – defined as a beneficiary’s Part A and B expenditures for affected months triggered by an inpatient episode of care for COVID-19. The same COVID-19 costs are removed from fee-for-service spending used to calculate regional and national trend factors. This will reduce the variation between the national and regional spending trends stemming from COVID, which will help large ACOs operating in COVID hotspots in particular.
In 2020, 37 percent of MSSP ACOs are subject to downside risk and will face potential penalties if their spending exceeds their benchmark. Prior to the new IFC, the proportion of ACOs with downside risk would rise to 64 percent in 2021. The new policy allows ACOs to continue in their current risk track for 2021, mitigating next year’s risk for many ACOs. The IFC also offers a one-year extension for ACOs whose agreement periods end in 2020 and allows them to maintain their prior benchmark.
Many ACOs have worked closely with their providers to rapidly deploy telehealth solutions after the Administration announced expanded Medicare coverage for these services. But CMS policy was unclear about whether telehealth visits could be counted for ACO attribution. The IFC clarifies that CMS will recognize many primary care services provided by ACO clinicians via telehealth, virtual check-ins, e-visits and telephone for beneficiary assignment starting in March 2020 and continuing through the public health emergency (PHE). This policy reduces the likelihood that 2020 ACO attribution will be skewed towards high-risk beneficiaries. But risks remain since it’s unlikely ACOs can completely make up lost primary care visit volume through telehealth; physician practices nationally have thus far replaced only fourteen percent of pre-COVID in-person visit volume with telehealth. ACOs also risk losing beneficiaries who receive telehealth services from non-ACO providers.
CMS previously established an “extreme and uncontrollable circumstances” policy that offered providers and ACOs certain regulatory flexibility in the face of emergencies like natural disasters. On April 6, 2020 CMS expanded this policy to provide relief to ACOs for any shared losses they incur based on the number of months the COVID-19 PHE is in effect. The May 8 IFC clarified that the COVID PHE officially began in January, and it was recently extended until July 21 by Secretary Azar. If the PHE ends in July, any ACOs incurring shared losses in 2020 would have to repay only 42 percent (losses forgiven for seven months out of twelve). If the PHE continues through 2020, all ACO shared losses would be forgiven.
Catalysis Healthcare Value Network member Torrance Memorial (TM) is a 610-bed hospital in California. Leadership, for years, has embraced respect for people as the principle underlying all their actions. It’s one thing to give lip service to “our people are our most important asset” it’s another thing to show it through action. When Covid hit Los Angeles, it was clear to leadership at TM adequate personal protective equipment (PPE) was going to be a big problem. At the same time there were staff who were idled by mandatory shut down of elective procedures. Leadership had to balance these two realities while maintaining the core of their belief system; respect for people. They came up with two core strategies. No layoffs and meet all PPE needs. A series of spectacular events transpired in which both strategies were realized. All PPE needs for the hospital were met and all employed staff kept their jobs if they chose to.
Jeremiah Hargrave is the PI leader at TM. His job radically changed in February. During the first few weeks of the crisis he, along with the Patient Safety Director Bret Barrett, was called upon to create a flexible labor pool. He became the manager. The goal: no layoffs, find meaningful work for everyone. Jeremiah immediately understood one of the top priorities; PPE. How could he leverage this pool of some 500 workers he had inherited who usually worked in outpatient surgery, GI, lab, and other departments? One of the flex pool nurse managers had an idea. She and her husband spent an evening at home building a face shield. The ICU was running low and there were none on boats from Asia coming any time soon. Using plastic laminate sheets in the garage they built a shield prototype. She brought it into the team the next day. They immediately recognized the importance of the discovery. After running it by infection control for approval the race was on to create a production process.
Jeremiah knows how to organize a team to build things, he worked at Toyota for 12 years prior to coming to TM to lead the improvement team. So, he worked with front line flex pool members to create an assembly line. The first team built 20 shields/hr. Then the PI team got involved. After multiple Kaizen they were at 130/hr. In three days, they built 5000 face shields meeting all the ICU needs. Every day they had different people. About 50 staff per day were working out of the flex labor pool. So, it was imperative to create standard work. Each day a training session took place for the new workers. Then a PI “supervisor” oversaw the worker until they understood the standard work and could complete it flawlessly. Without standard work there is no way they could have trained so many staff in such a short time to produce that many masks. Think of Rosie the Riveter. During world war 2 untrained workers used standard operating procedure manuals to quickly learn standard work which allowed for ramped up production of the materials required to win the war. Covid is a different kind of war but the core of lean thinking still applies.
Another problem arose. The organization was running out of sanitary wipes. Again, with supply chains in shambles the PI team and flex pool staff were called on to quickly figure something out. Someone from environmental services said, “we have oxycide disinfectant can we use that”? Quick study showed the disinfectant could be used to saturate microfiber cloth. The individual cloth squares once saturated could be bagged up and sent to units. Within a day or so a mothballed medicine unit was opened, supplies were gathered, and the process was started. The flex pool employees were assembled again following standard work and within two days they were producing 100 bags with 12 wipes each a day. A bonus, the cloths could be reused!
Other meaningful and important work was created for these employees. They screened employees and patients as they entered the hospital for symptoms, including taking temperatures. Who knows what’s next, but this team of people led by great leaders feel they can tackle just about anything at this point?
There are many lessons we can learn from this amazing example of leadership and creativity. Let’s summarize into 5 questions all healthcare leaders should be asking themselves now.
Where is the principle of respect for people on your priority list?
What goal have you set for number of staff infections?
Have you created any alternative other than laying idle staff off? If so, what?
Have you supported and re-deployed staff to do work that gives their life meaning? How do you know?
What process is in place to unleash the creativity of staff to solve problems?
What will you learn from the TM example? Someone once famously said “don’t let a good crisis go to waste”. Maybe it’s time to rethink the underlying principles of your work. Or establish a management system for improvement or re-examine what metrics you are tracking. Whatever it is, do something to improve yourself and your organization. A good start is to begin to answer the five questions. You can build a better future for your people, now is the moment to make lasting change happen.
There was no script or plan etched in stone that had simple answers or even protocol as potential supply shortages loomed ahead of WellSpan Health’s COVID-19 journey.
Instead, leaders within the organization took a proactive approach by fostering relationships to secure necessary resources needed to care for communities and staff, including a special partnership with Letterkenny Army Depot near Chambersburg, Pa.
On May 1, Letterkenny started production of 70,000 protective gowns for WellSpan Health to help bolster the local health care system’s supply chain as it continues to navigate through the COVID-19 pandemic. In addition, Letterkenny produced prototypes for cloth face masks for WellSpan Health which has shared the designs with other community partners.
“The level of community engagement and support of the health system in an unselfish manner has been overwhelming. Letterkenny has been the epitome of that,” said Keith Noll, senior vice president – chief administrative officer for WellSpan Health.
No matter the stage your organization is in during the COVID-19 pandemic, the rapid changes and new challenges in this crisis can easily derail people. So how do you get your teams back on track?
Recently, Kerri Burchill, PhD, Organization Development Leader from Southern Illinois Health, one of our Catalysis Healthcare Value Network members, shared four strategies to help guide people back on track.
At Seattle Children’s, the Improvement and Innovation Department is driven by their commitment to helping faculty and staff find new and better ways to serve their patients, families, and team members. This shared resource spans the organization and includes services such as coaching, consulting, design engineering, education, project management, and simulation. Amidst the COVID-19 pandemic, the team’s work has shifted to help overcome potential equipment shortages in personal protective equipment. A recent example illustrates how the team collaborated to meet the demands of fast-changing clinical workflows that taxed the supply of Controlled Air Purifying Respirator (CAPR) helmets. What could have turned into a serious safety issue, instead became an innovation story with a fairytale ending.
UMass Memorial Health Care has taken a financial beating during the coronavirus pandemic, as it, like other hospital systems, has forgone revenue-generating procedures during the outbreak.
But the Worcester-based system is committed to not laying off or furloughing any workers despite the financial hit, President and CEO Eric Dickson said in a staff memo Wednesday.
“While this decision to retain our caregivers did increase pressure on our financial health, we as a senior leadership team – with the endorsement of our board of trustees – felt that was the right thing to do,” Dickson wrote.
Catalysis faculty member and author of Patient-Centered Strategy, Jeff Hunter to discuss some of the questions that he has been hearing from healthcare leaders on how COVID-19 is and should impact their strategy deployment process.
The know-how Stefan Metzker gained on his journey – first as a Cape Town intensive care doctor, then supplying African doctors with Chinese-made surgical gear and now as a Swiss hospital CEO – prepared him to help when COVID-19 struck.
Answering a call from Zurich officials desperate for face masks, surgical gowns and gloves, Metzker leveraged a Chinese business contact he had forged decades ago to secure 23 million items of medical gear.
Since April, passenger-turned-cargo jets belonging to Lufthansa unit Swiss Air Lines have made 15 non-stop flights from Shanghai to Zurich.
Like many healthcare organizations across the United States, INTEGRIS Health, in Oklahoma, had many questions about how to prepare for COVID-19. How would the spread of the virus look in Oklahoma? Were they prepared for a surge of COVID positive patients? How were they going to manage and handle these patients, as well as other activities within their hospitals?
The extremely contagious nature of COVID-19 during certain procedures led a Mercy team to create a new operating “bubble” that allows surgeons to perform an open tracheostomy on the sickest patients without moving them to the operating room.
Tracheostomy is high risk for the surgery team because of the aerosolization that occurs when a breathing tube is inserted into the windpipe. The procedure becomes necessary when very sick COVID-19 patients spend prolonged time on a ventilator. It protects their vocal cords and makes it safer to wean them from breathing support when their condition improves.
“We move the OR to the intensive care unit,” said Dr. Alison Gildehaus, medical director of trauma and acute care surgery at Mercy Hospital St. Louis. “Patients stay in their negative pressure, ICU rooms – removing the added risk of transport – and the surgery team comes to them. We limit the number of people in the room, thus conserving PPE, yet have added support right outside.”
This is the fourth edition in a series of write-ups on innovations that Mount Sinai Morningside hospital has implemented during the COVID-19 pandemic in New York City. We hope you find the accounts of our agile response useful and we encourage you to reach out with any questions. Contact information provided at the end.
Mount Sinai Morningside Hospital in New York City has built a culture of improvement on a foundation of principles. In this podcast Maytal Rand, Emergency Manager, shares the story of their Haircuts for Heroes program. This is just one of the ways that they are showing respect for their staff during the stressful time COVID-19 has presented. This story presents evidence of their strong culture and principle-based leadership.
Hospitals and health systems in the U.S. are balancing clinical and workforce priorities as they experience the effects of the COVID-19 pandemic and plan for what’s next.
Executives have adjusted their strategies and operations to ensure patients receive quality care and that employees are supported mentally and emotionally. Here, nursing leaders from hospitals and health systems in some of the states hardest hit by the public health crisis share their top priorities and advice for colleagues preparing for a surge of COVID-19 patients.
Mount Sinai Health System announced Thursday launch of the Mount Sinai Center for Stress, Resilience and Personal Growth, a first-of-its-kind initiative in North America designed to address the psychosocial impact of COVID-19 on the mental health and the lives of frontline health care providers at Mount Sinai.
“Mount Sinai’s doctors, nurses, trainees, students, and clinicians and support staff are on the front lines of the battle against COVID-19, healing as many people as possible, yet they are witnessing death on a scale no one should ever have to endure,” said Dr. Dennis S. Charney, the Dean of the Icahn School of Medicine at Mount Sinai and President for Academic Affairs for the Mount Sinai Health System.
“Many are absorbing the anguish of patients’ final hours, serving as a lifeline for patients and families who are unable to be at the bedside, while facing personal danger and the ever-present risk of becoming infected themselves to the virus,” Charney went on to say.
Article from Modern Healthcare featuring work from Catalysis Healthcare Value Network member, Cleveland Clinic, and sponsor memeber, Epic.
Cleveland Clinic worked with Epic, its electronic health record vendor, to develop and implement a COVID-19 home monitoring program that is now available for other healthcare organizations across the country to use.
Collaboration among clinicians and analysts helped the Clinic to rapidly design, build and launch the technology in just 10 days. Typically, it would have taken three months to do so, said Dr. Eric Boose, associate chief medical information officer at the Clinic.
Though patients with COVID-19 often experience mild symptoms, monitoring these symptoms is critical because deterioration can be rapid, even in low-risk patients. The new tool automates patient engagement and supplements existing processes to enable the Clinic to extend the reach of clinicians without adding staff members, according to a post on Epic’s Health Research Network.
Rush University Medical Center shares their latest surgery restart guidelines. This may be helpful to others as hospitals try to determine what processes, systems, and materials need to be in place to restart surgeries.
Early into the evolving response to the COVID-19 pandemic, Rush University Medical Center’s Chief Wellness Officer Bryant Adibe, MD, commissioned a special Wellness Task Force. This task force was devoted to coordinating Rush’s efforts as part of the overarching command center structure. With its collective expertise, the task force created five key mitigation tactics to reinforce well-being throughout the crisis.
“We know outside of a pandemic, health care workers are already at a high degree of risk for burnout and other issues around their well-being,” said Dr. Adibe, vice president of Rush University System for Health in Chicago. “We recognized it was really a priority to make sure that the well-being and mental health of our front-line workers was getting prioritized and ensuring that we had an organizational infrastructure in place to not just get through this crisis, but to ultimately allow our community to thrive.”
The Federal government has made funding available for healthcare organizations fighting COVID-19 from the SBA, FCC and FEMA. Jane Jerzak and Kim Heller with Wipfli CPAs and Consultants will present the most current information and answer questions.
There is great concern throughout the U.S. that health systems will not be able to meet the demand of the potential exponential growth of critically ill patients with COVID-19. This is playing out in New York where some hospitals have full ICUs and too few ventilators to meet the patient demand. Many of these hospitals are in a crisis management mode yet only a few, such as Morningside Mt. Sinai (listen to our podcast), have actually built a standardized management system that can support the front line in this crisis. In other parts of the country there are shining stars that have been building a standardized management approach that has readied them for just such a crisis. In Cleveland, Ohio, the Cleveland Clinic provides nearly 10 million patient visits a year. Leaders and staff there recognized the gravity of the situation at the end of February and acted quickly and decisively to help stave off the chaos that is now crippling other health systems.
For years Cleveland Clinic has been on a journey to excellence. It has built a series of standardized systems that are based on the core principles of organizational excellence. Principles such as respect for people and pursuit of a “culture of improvement,” which has led to engaging employees (“caregivers”) in everyday problem solving. A core principle to Cleveland Clinic’s work has been using scientific problem-solving methods to identify and solve difficult problems. Over 20,000 Cleveland Clinic employees have been trained to use scientific methods to tackle all kinds of daily issues, drive innovation, and maintain stability.
So COVID-19 was a new problem – a new and particularly challenging problem – that staff unleashed their problem-solving skills and creative ideas to solve. Supported by a robust improvement system, these ideas could be rapidly and effectively trialed and have led to some remarkable almost overnight changes.
Cleveland Clinic is guided by an overarching “True North” – a clearly articulated purpose that drives all decisions: Serving our patients and our caregivers. This focus helps to provide clarity in decision-making every day and has been the overarching guide to attacking COVID-19.
Leaders at Cleveland Clinic have looked at serving caregivers in terms of the needs they have for information flow, equipment, and support. One of the many systems created to achieve True North is a management system that involves tiered daily huddles. Since their inception in 2018, tiered huddles occur each day across the enterprise at every level from CEO to “bedside” teams. In the case of COVID-19 this system allowed for rapid capture of critical operational information across large, geographically separated business units (hospitals and outpatient facilities) in order to identify and solve problems quickly at all levels of the organization. The huddles disseminate information, updates, gratitude and support – consistently, and rapidly. COVID-19 required rapid updating of the standard content of every huddle to include information on staffing, the number of patients testing positive in the hospitals, in which units they were being cared for, and the number of persons under investigation at any given time. Since these huddles were developed and standardized long before the crisis, changes could be rapidly implemented and backup was in place for times when the huddle leader was pulled to other COVID-19- related activities. In addition, now some teams are huddling virtually because a number of people are now working from home for “social distancing.” Although the virtual huddle is new for many, the Cleveland Clinic staff are quickly learning a lot about how to do that effectively.
The result of rapidly cascading management decisions has included the rapid implementation of drive-through testing sites for COVID-19. This was initiated on March 14, one of only a few of the first drive-through testing sites in the nation. Since then public health departments and other health systems have copied it. The process is designed to test patients in a “drive-through” fashion, in a car, while keeping patients and caregivers safe. The improvement teams worked with staff and leaders to develop a new process and use rapid cycle kaizen to improve from 30 to 115 patient samples collected per hour over the first five days with the same staffing. Staffing the drive centers was a challenge and improvement teams came up with ideas such as staffing the site with volunteers from multiple locations, functions, and skill sets including people with clinical and nonclinical backgrounds. Staff were quickly trained and integrated into the process of safely registering a patient, doing a nasal swab, and safely packaging it for transfer to the lab – all while maintaining safety precautions to protect both the patient and the caregiver.
The importance of staff safety in this scenario cannot be overstated. If staff aren’t safe patients aren’t safe. A recent article in Bloomberg news tells the story of caregivers going to Home Depot to construct their own masks. The supply chains in the U.S. are not keeping up with needs for our staff to be safe. Leaders’ No. 1 priority must be safety. In another example a colleague and primary care doctor in Wisconsin is taking the mask he uses during the clinic hours and placing it in a Tupperware container at night not knowing if he will have access to a fresh mask in the morning. Tiered daily huddles and gemba walks enable leaders to deeply and rapidly understand the challenges faced by staff and patients in outpatient clinics, emergency departments, and hospital floors. Safety remains paramount, and leaders must remove barriers quickly on issues and questions arising from the front line as Cleveland Clinic does with daily tiered huddles.
Cleveland Clinic’s improvement team has been redeployed to help leaders and front-line team members map existing processes and create new future state processes, and scientific problem solving, visual management and standard work are broadly applied at the hospital’s command centers. This thinking will be required to rapidly assess patient demand, resource needs and staffing as well as to triage patients while keeping our patients and caregivers safe.
We know for certain that we will need the ideas of every caregiver, manager and leader at Cleveland Clinic to identify and solve the many new problems that arise in this crisis. But by applying the new standard work processes created from rapid improvement cycles and continuing to encourage all staff to experiment with novel ideas not thought possible before, Cleveland Clinic staff and leaders are confident this challenge will be another problem that can and will be solved.
This is the third edition in a series of write-ups on innovations that Mount Sinai Morningside hospital has implemented during the COVID-19 pandemic in New York City. We hope you find the accounts of our agile response useful and we encourage you to reach out with any questions. Contact information provided at the end.
In early March of 2020, the Mount Sinai Morningside (MSM) Incident Management Team (IMT) was activated to support the hospital’s response to the COVID-19 pandemic. Within a week, our census of patients who were either diagnosed with COVID-19 or under investigation for COVID-19 (PUI) doubled, then tripled, then increased exponentially. The IMT focused on strategies to maintain isolation of these patients.
We are working with organizations in our healthcare community to understand the process and needs for restarting business lines in healthcare organizations as many healthcare organizations are thinking into the future. Here is the most recent guidance and thinking.
Update 04-28-20
How much COVID-19 space is necessary?
Are the expanded spaces held in reserve or put back to prior use?
Do you prepare the expanded spaces with things like permanent oxygen and sinks?
Meet with front-line staff to get ideas on
New huddle topics
Safety standards
Remove new processes implemented that are not adding value
Adjustments to staffing
How do you safely restart your cafeteria service?
How will ancillary services safely deal with COVID & non-COVID patients?
PT, OT, Imaging, etc.
Waiting areas need to be sanitized regularly
Communicate COVID scheduling changes with referring and admitting practices
Do you need a dedicated communications person/team for partners?
Establishing a Governance Council for decision making still harder than it seems
Update 04-27-20
Create a staffing plan six weeks out. Your team will need a break. Even those coming off a furlough will find stress in the new COVID-19 environment.
Collaboratively create a “Go/No-GO” checklist.
Staff are experiencing trauma and it is incumbent upon all of us to provide counseling and needed care.
New sanitation processes need standards. Staff need to be trained. Inspection is mandatory.
Create messaging & signage on why patient PPE is important
Plan the Command Center wind down. Do not totally dismantle
Get back to SAFETY. Many safety processes have been bypassed or ignored for all the right reasons.
Prioritize and stabilize versus solving all the problems at once.
Set new goals and targets. Track and measure. Celebrate successes
Closely monitor the supply chain. Validate delivery dates and accurate received quantities. Do not let safety stocks diminish.
Identify skills that were in short supply during the last surge. Create a plan to train up and expand capacity
Leadership get involved: What is your safety stock quantities and how were those calculated?
Restart Planning Notes 04-23-20
Number 1 priority: Establish a Governance Council
Becker’s recommend 6 P’s for the Governance Council
Plan (Develop one)
Policy (Know policy & regulations)
Procedure (Track backlogged procedures/visits)
Process (Design new processes and protocols)
Place/PPE (Set Place & PPE standards)
Patient (Engage the patient)
Number 2 priority: Apply for PHSSEF Grants ASAP
Priority 3: Restart plans have to include the fact that COVID-19 will be here for a while
How do you bring back furloughed staff?
Some may now have daycare issues trying to send their kids back
HR coordination necessary
Union seniority a consideration?
License/certifications current and not elapsed?
Training on new procedures
Training on COVID-19 Patient Care
What are the new procedures for patients?
Patient arrival
Patient waiting room distancing
Family/visitors
Recovery
Discharge
Communication plan for patients, family & staff
Scheduling
How to deal with COVID-I9 testing prior to surgery
How to get pre-authorizations done ahead of time
How to validate patients still covered by insurance (laid off?)
Do you have enough schedulers and phone call capability?
How to communicate with surgeon’s clinics
How to communicate new safety procedures
Safety
Intubation may require less staff around patient
What are the new processes/standards?
Will it take longer for each procedure due to new safety protocols?
PPE Stocks
COVID-19 PPE needs for patient flow will continue for ambulatory, drive-thru clinics, inpatient procedures and now outpatient procedures
What are your safety stock percenages?
How did you arrive at that? Hopefully using standard deviations
Built the appropriate safety stock for:
Current patient flows
New patient flows
A fall pandemic
What is your forecasted PPE usage vs your actual PPE usage each day?
PDSA
Increased PPE demand beyond historical use for outpatient procedures
Staff sanitizer including office staff
Are dominant areas appropriately sanitized for the restart?
Is all equipment current for calibration and certification?
Is a local Safety Officer necessary for the initial restart?
How do you communicate to patients about safety and their concerns?
Surgery Centers & clinics: if a patient has to be admitted, are you familiar with the hospital’s new protocols?
What is the plan if a “spike” or “mini-surge” occurs and you must defer again?
As we have battled the COVID-19 crisis, a few of you have had the experience of knowing someone who has been afflicted with this disease. Some of you have already watched loved ones struggle to recover, while others have experienced devastating losses.
For me, that wasn’t the case until last Friday when COVID hit home.
Jane Jerzak, a partner with Wipfli, CPAs and Consultants, shares funding opportunities that are available for healthcare organizations to help with the significant financial burden that the COVID-19 is causing. Jane works with healthcare organizations in both larger communities and rural settings.
These Treatment Guidelines have been developed to inform clinicians how to care for patients with COVID-19. Because clinical information about the optimal management of COVID-19 is evolving quickly, these Guidelines will be updated frequently as published data and other authoritative information becomes available.
The recommendations in these Guidelines are based on scientific evidence and expert opinion. Each recommendation includes two ratings: a letter (A,B, or C) that indicates the strength of the recommendation and a Roman numeral (I, II, or III) that indicates the quality of the evidence that supports the recommendation (see Table 1).
Health systems continue to grapple with the clinical and financial implications of widespread COVID-19 cases, with a new focus on preparing for the future.
Health IT leaders are collaborating to open field hospitals and work together on technology that will track the symptoms and spread of COVID-19 after stay-at-home orders are lifted and states reopen. Big tech companies are making even more data available than in the past to help health systems plan for resource allocation in the future, and new cybersecurity threats are emerging.
COVID-19 spread has put an overwhelming strain on the resources and personnel of New York City healthcare institutions, as the region surpassed 120,000 confirmed cases this week—now making up approximately 20% of all cases in the US.
The need for not only frontline tools and therapies but fallback options has forced caregivers to seek outside funding and donations—and to consider innovations of their own.
A team of anesthesiologists, pulmonologists, sleep and critical care specialists, and medical students at the Mount Sinai Health System have found the replicable means of reconfiguring donated variable positive airway pressure (VPAP) machines originally designed for sleep apnea care into ventilators for use on the most severely ill patients hospitalized with COVID-19 in the city.
The fallback ventilator option is now being documented for production and use, to be shared with communities and institutions similarly burdened by high patient counts and limited resources.
Telemedicine has quickly become a reality in many health systems as healthcare providers work to meet the needs of their patients while keeping them same from the coronavirus. Here are some tips that might be helpful.
While there is no off-the-shelf playbook for the current coronavirus pandemic, existing management research points to ways that organizations can navigate tumultuous and uncharted times through innovative strategy and creative tactics. This article outlines five actions that should be taken by health care leaders: put people first, manage operations creatively, attend to teamwork and communication, create outside partnerships, and embrace clear and humble leadership.
Many healthcare professionals are experiencing pressure injuries from the use of PPE. Here is some standard work that Children’s Mercy Hospital shared with us on how to prevent those injuries.
As everyone has become painfully aware, acute shortages of materials like masks, ventilators, intensive care unit (ICU) capacity, and staff are hamstringing the heroic efforts of health care professionals around the world to address the pandemic.
Now, more than ever, the right supply-chain strategies and management practices are urgently needed to optimize scarce resources, alleviate shortages, and expand capacity quickly. While good management can never be a substitute for dedicated and skilled medical practitioners, improving the management of supply chains is crucially needed to ensure that these professionals have the resources to do their jobs.
This article, which draws from the best practices in supply chain and operations management, can help struggling hospitals and other care providers increase the odds they will have those resources. It is based on a central reality: Tackling shortages and supply constraints requires a comprehensive strategy aimed at both the demand- and supply-side roots of the problem.
Eric Dickson, MD, President and CEO at UMass Memorial Healthcare, values his team of problem-solvers who have banned together as an army in the war against COVID-19. Read his thoughts in his blog post about how UMass is working through this pandemic.
From our many discussions with Catalysis Healthcare Value members and healthcare organizations around the world we have been gathering information and documenting to help your organization prepare for the COVID-19 surge and the future restart of healthcare operations.
We will keep this checklist updated as we obtain more information.
A Vice President of Process Improvement and a Lean Specialist are managing the day-to-day process development, questions fielding, and workflow development for:
Workflow and criteria for COVID-19 testing for physicians and providers
Database and process for notifying physicians and patients of results
Infection control processes and workflows, including PPE standards, education, and electronic mechanism for observations by PPE Evaluation Personnel (PPEEPs)
PPE conservation practices and processes, including monitoring by PPEEPs ensure compliance; supplies inventory updates 2X day
Process for donations of PPE, sources, and resources for emergency backup options, such as handsewn items
Visitor policies and restrictions, including the screening criteria and processes
Patient/Family communication process with passcodes
Ongoing labor pool resource and database process
MD/provider hotlines (ring into Command Center) for vetting testing criteria and process
COVID unit patient placement, maps, and flow
Process for “call ahead” for positive patients coming to the ED after a positive result
Leader and coworker hotlines (ring into Command Center) for vetting FAQs (to relieve Employee Health and Infection Prevention nurses)
Assistance with process/workflows for offsite testing and evaluation sites
Manage daily updates documentation for Leaders group and for daily 3pm call
Monday/Wednesday/Friday 7:45 am webx for larger leaders group communication
Signage creation and lamination, and other visual management for visitors, screening, restrictions, hand hygiene, etc.
Management of vital phone numbers
The modified command center is staffed from 7a-7p. In addition to the VP and Lean Specialist, hospital directors serve in the command center for a 6 hour shift from 7a- 1p and another from 1p-7p.
Resilinc and Premier Inc. to Launch Healthcare Exchange to Help Hospitals Access Supplies and Ease Shortages During COVID-19 This is a collaboration with “Stanford Medicine to bring the Exchange from concept to reality, leveraging our experience in helping our customers protect their supply chains from disruptions.”
Providers can apply to join The Exchange in under 10 minutes by clicking here, and each provider can list items it needs and offer those it can spare in exchange. Healthcare organizations, nonprofits and other businesses are encouraged to apply if they would like to donate much-needed supplies.
The following is intended to be a resource to hospitals and health systems regarding pertinent funding included in federal COVID Legislation, and from other sources as appropriate. As additional information becomes available this list and the attached tables will be updated. These funding sources may include certain restrictions, interest, and requirements. We recommend that anyone using this document consult your CPA firms for additional information and specific guidance.
Programs Available to All Eligible Employers
1. Payroll Tax Delay
2. Paycheck Protection Program/SBA Loans
3. Economic Injury Disaster Loan (EIDL) and Economic Injury Grants
4. Employee Retention Program
5. Other Business Loans through the Federal Reserve
Programs Specific to Health Care Providers
1. Accelerated Medicare Payment Program
2. The $100 billion Fund” – Funding from the Public Health and Social Services
Emergency Fund
3. DRG Add-On for Inpatient Medicare Services
4. Medicare Sequester Extension
5. Extension of the Work Geographic Index Floor
6. HRSA Funding for Rural and Critical Access Hospitals
7. State Hospital Association Grants to Hospitals
8. Telehealth Networking Grant
9. Distance Learning and Telemedicine Grant
10. COVID Telehealth Grant
11. Medicaid DSH Reduction Delay
Other Funding Possibilities
1. CDC Funding
2. FEMA Grant Funding
Brian Radbill, Incident Commander and CMO, and Art Gianelli, President, from Mount Sinai Morningside Hospital in New York City. Being in New York City puts them at the heart of the crisis. They share what they are doing to support front line staff, how their improvement team has supported the organization during this time of crisis, as well as what systems they have put in place that have been particularly valuable in the fight against COVID-19.
Lucy Xenophon, Chief Transformation Officer, Brian Radbill, Incident Commander and CMO, and Art Gianelli, President, from Mount Sinai Morningside Hospital in New York City share their learing from the COVID-19 pandemic. Being in New York City puts them at the heart of the crisis. Hear about the current state at the hospital as well as advice they have for preparing for a possible surge of COVID-19 patients.
Rush University Medical Center, a member of the Catalysis Healthcare Value Network, shares a playbook for navigating clinical and operational challenges of a global healthcare crisis.
Coronavirus has disrupted supply chains for 100% of US companies. In this white paper produced by LeanCor Robert Martichenko discusses the impact in a post COVID-19 world.
Memorial Sloan Kettering Cancer Center from Dr. Lee Erikson
Set up a Coping with Stress Hub on our intranet
Communicated widely about our EAP mental health resources
Set up several on line resources with links to apps for meditation, mindfulness, exercise, tai chi, etc.
The psychiatry department is offering telemedicine counseling sessions to staff
Launched a series of short self-care videos
Lurie Children’s from Laura Westley
It really is a challenge. To date, the impact of COVID19 to Lurie Children’s has been a dramatic decrease in census- we are currently at a 60% census point vs. the 90% just a few weeks ago. Our facility had been cancelling 30-40 nurses on a daily basis. Our adult facility partners are in a much different position currently, however everyone is impacted by the constant messaging/ reporting in the media.
Our organization has been in Incident command for nearly 4 weeks, I will review a few things we have in place, in no particular order. I hope some of it may be helpful.
Incident Command
Each meeting begins with a current state of our local pandemic- #tested, those +, etc. The actual numbers have been helpful to gain perspective
Daily reports from incident command with a general overview sent as a global message throughout the organization
Directed messages to leaders in the various areas of the organization
My areas fall under the operations function of incident command. We receive a more detailed summary of discussion points before changes have been implemented. These are shared with area leaders who use them as discussion points with their teams. Any specific questions are then returned to incident command for review and are typically responded to within the same day.
Weekly virtual Town Hall meetings facilitated by the CEO have been in place since we have been in incident command- about a month.
These have been augmented by additional virtual Leadership Town Hall meetings, facilitated by some of our executive leaders, intended to help leaders better support their teams
To date, topics have included HR issues and questions
Change management
Next week will feature our psych team talking about personal resiliency
The organization has an “ALL Connect” site intended to be an all-inclusive site for resources
HR links with information as people are furloughed
Current screening information
Links to CDC and IDPH for up to date broad view information
COVID19 email link has been created for staff to ask questions- many times they are themed and used for upcoming Town Hall topics
Marketing and PR team is represented in Incident Command and are responsible for creating global messaging for the organization and community
COVID19 link on the organization web site-
The messaging has been heavy on the value of the care provider and the intent to keep them safe. Departmentally, it has been helpful to group messaging to minimize a potential overwhelming impact to staff. Visibility, availability, and timely response have been most effective.
The COVID-19 pandemic is causing shortages of PPE, meaning that healthcare organizations all over the world must finding creative ways to help ensure that their staff has what they need to effectively care for patients.
Catalysis Healthcare Value Network member, Torrance Memorial Medical Center, in Torrance, Ca, formed an assembly line to produce face shields for those on the frontline. The idea came from a nurse who was trying to figure out how she could help contribute to the COVID 19 work. They staffed this assembly line with employees from all across the organization including physical therapy, occupational therapy and nursing, and came up with a process to use laminating sheets, kanban and foam. Jeremiah Hargrave, Manager Process Excellence and his team helped get the line up and running at the start and it was not much later that they were engaging the team to find improvements to the process.
The first day the team was able to make 100 face shields in 3 hours. After some PDSA of the process they adjusted and were able to assemble 120 face shields an hour with the same amount of people and following social distancing rules.
Great job Torrance Memorial! This is a great way to put your lean knowledge and other resources to use to provide value to patients during the COVID-19 crisis.
The CDC has published a PPE Burn Rate Calculator to help healthcare organizations estimate how long the current stock of PPE with last and give an idea of what to order to be prepared for future needs.
Mount Sinai Morningside is a hospital in New York City. They have put a lot of standard work in place while learning on the fly as the surge of COVID-19 patients hits in New York. They would like to share what they have in hopes that it can help other healthcare organizations preparing for the possible surge of COVID-19 patients in their areas.
The COVID-19 pandemic has changed lives for everyone across the globe and has hit the healthcare industry hard. Our Catalysis Healthcare Value Network members have shared a lot of standard work and other information with us that can be helpful for hospitals all over the world.
We are grateful for the hardworking healthcare professionals who are working tirelessly under difficult circumstances. Catalysis is working to bring together resources to help our community learn, share, and connect around navigating through the COVID-19 pandemic. Catalysis will do all we can to leverage our resources and network to be part of the solution to this crisis. You can access resources on our website, createvalue.org, on the COVID-19 Resources page.
The Covid-19 pandemic is pushing healthcare systems around the world to the limit and, despite the heroic effort of healthcare professionals, hard work is often not enough. The images coming from the most heavily affected areas tell us of Emergency Departments filled to the brim, hospitals struggling to treat everyone due to the very high number of people that the virus sends to the ICU, and exhausted staff who are often forced to work without adequate protective gear.
Over the past several weeks, the COVID-19 pandemic has challenged routines in all of our lives and has brought into focus the need for rapid change as we race to re-define and improve how we are delivering health care. At Mount Sinai Morningside (MSM), an urban community hospital in New York City and a member of the Mount Sinai Health System, we have started up a traditional incident management team (IMT), including an Incident Commander and Section Chiefs for Planning, Operations, Logistics, Safety, Medical Specialty, Finance, and Communications. In addition to the traditional structure, we have connected real-time data and rapid tests of change to our incident command response.
The IMT hub of operations is The James Jones Daily Management and Incident Command Center (DMC). The DMC, created in 2018, houses 10 digital dashboards which display real-time information for both clinical and non-clinical operations, pulled directly from our electronic health records. The data displayed on the dashboards were chosen by numerous facilitated interdisciplinary design workshops. Since inception, the information from the DMC has been connected to daily management and standard work. One of the dashboards is reserved for emergencies and is known as our Disaster Tile. Since opening the DMC, we have practiced using this dashboard for mock mass casualty events but are now using it for real-time management of our COVID-19 response. The IMT huddles multiple times daily and reviews the information below, which has now been added to the Disaster Tile:
Total number of COVID-19+ patients and their bed location (ICU, non-ICU, and ED)
Total number of Persons Under Investigation (PUI) and their location
Total number of COVID-19 or PUI patient expirations (ICU, non-ICU, and ED)
Total transfers from ICU to non-ICU and vice versa
Total discharges to home or other facilities
Total number COVID-19 tested (Admitted, Discharged, and Admission Decision Pending)
Total number of ED patients ordered to self-isolate but not tested
Number and location of negative pressure rooms
Total number of surge critical care beds and occupancy by location
Total number of surge non-critical care beds and occupancy by location
Total number of patients on invasive and non-invasive ventilation
Since we do not have an electronic process that connects to our morgue, we review but must manually account for census and LOS for decedents.
In addition to connecting our information framework to our incident management, we have been actively engaged in numerous rapid tests of change to solve issues identified in the command center. As problems are identified, a workgroup of stakeholders is quickly convened in the Lean lab and solutions are identified within one-two hours. The solutions are presented to the IMT for awareness. The Lean team has taken an active role in operationalizing the process changes with the appropriate stakeholders, shifting from our usual coaching/teaching model.
It is impossible to catalogue all of the rapid cycle PDCAs that have occurred. In one example, early in our journey, we needed a solution for protecting resuscitation teams attending to patients with unknown COVID-19 status. Our solution was a PPE “go” bag. We have included the specifics of this tool/workflow and a few other tools and process changes in the link below. As the pace quickens and our needs evolve, much of our work is already outdated, however, we hope that by sharing some of the changes made, we can inform and inspire other process improvement teams who are on this same journey across the globe.
The tiered daily huddles still occur as usual (same time, same people (with the caveat that every leader is responsible for having someone else ready to fill in if he/she is busy – that’s not new). The content has shifted to systematically include content around COVID – like # of “persons under investigation (pending COVID test results) and # of COVID positive patients in house and where they are (regular floor or ICU, etc.) for each. Also, trying to understand our staffing – # caregivers out, # caregivers positive, the impact, and any operational issues/concerns/questions.
These metrics are reviewed For each hospital – then all hospitals report in for Tier 5 – and the entire system is reviewed in Tier 6 –which the CEO runs.
The IC Process is separate. Complicated problems that are elevated through the tiered daily huddles go to the IC for recommendations, which are then approved (or not) by the Exec Team.
Mercy St. Louis shares how their PI Team is helping in this time of crisis.
A Vice President of Process Improvement and a Lean Specialist are managing the day-to-day process development, questions fielding, and workflow development for:
• Workflow and criteria for COVID-19 testing for physicians and providers
• Database and process for notifying physicians and patients of results
• Infection control processes and workflows, including PPE standards, education, and electronic mechanism for observations by PPE Evaluation Personnel (PPEEPs)
• PPE conservation practices and processes, including monitoring by PPEEPs ensure compliance; supplies inventory updates 2X day
• Process for donations of PPE, sources, and resources for emergency backup options, such as handsewn items
• Visitor policies and restrictions, including the screening criteria and processes
• Patient/Family communication process with passcodes
• Ongoing labor pool resource and database process
• MD/provider hotlines (ring into Command Center) for vetting testing criteria and process
• COVID unit patient placement, maps, and flow
• Process for “call ahead” for positive patients coming to the ED after a positive result
• Leader and coworker hotlines (ring into Command Center) for vetting FAQs (to relieve Employee Health and Infection Prevention nurses)
• Assistance with process/workflows for offsite testing and evaluation sites
• Manage daily updates documentation for Leaders group and for daily 3pm call
• Monday/Wednesday/Friday 7:45 am webx for larger leaders group communication
• Signage creation and lamination, and other visual management for visitors, screening, restrictions, hand hygiene, etc.
• Management of vital phone numbers
The modified command center is staffed from 7a-7p. In addition to the VP and Lean Specialist, hospital directors serve in the command center for a 6 hour shift from 7a-1p and another from 1p-7p.
MDmetrix is offering COVID-19 Mission Control to hospitals subscription-free nationwide. This works with your internal EMR, so some IT support would be necessary to get it in place. Dan Low, Chief Medical Officer and anesthesiologist as Seattle Children’s shared with us “We need help giving this away faster – before the storm hits full force.”
The Permanente Medical Group has set up an incident command center to provide structure and a framework for managing in a crisis situation. Their entire management system has shifted to COVID-19, including daily tiered huddles and stat exchanges.
The process uses vaporized hydrogen peroxide to kill germs without degrading the masks
DURHAM, N.C. – Facing a critical shortage of N95 face masks that block the coronavirus, Duke Health research and clinical teams have confirmed a way to use existing vaporized hydrogen peroxide methods to decontaminate the masks so they can be reused.
The process uses specialized equipment to aerosolize hydrogen peroxide, which permeates the layers of the mask to kills germs, including viruses, without degrading the mask material.
I realized when I was in graduate school that I needed to understand the concepts I was learning inside and out and be able to practically apply them, because this would be the work I would be doing for my career. I couldn’t simply memorize information to pass my tests, I needed to alter my thinking.